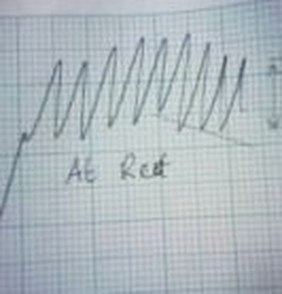
Figure 2 - Spirograph of Breathing Rate at Rest
|
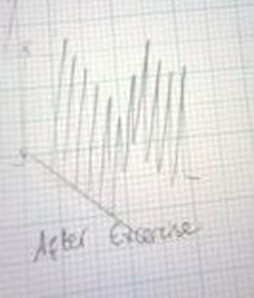
Figure 3 - Spirograph of Breathing Rate After 1 Min Exercise
|
Practical Investigation into the Effects of Exercise on the Respiratory System
Aim
To investigate how exercise affects breathing rate and how aerobically we do so by monitoring a test subject’s breathing rate at rest and after exercise and analysing spirometer results.
Method and Apparatus List
- Spirometer
- Stop watch
- Test subject
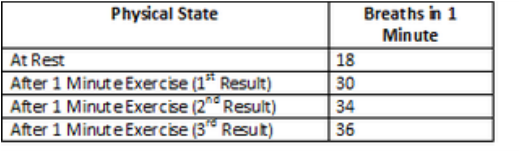
First we measured our test subject’s breathing rate for 1 minute when they had not been doing any exercise using a spirometer. We then had her jog on the spot for 1 minute and measured her breathing rate via the spirometer again. Counting the number of waves which were produced on the Spiro graphs allowed us to work out how many breaths the test subject took in each instance during each minute. Unfortunately the temperamental nature of the spirometer meant we had to take our further results manually. We allowed our test subject time to recover from the first minute of exercise before asking her to jog on the spot for another minute. We counted her breaths for one minute afterwards, then allowed her to rest again. Then we asked her to jog on the spot one final time and counted her breaths for the minute after and entered our results into a table as in figure 1:
Results
Figure 1 – Table of Results
Conclusion
We can draw several pieces of key information from comparing the 2 Spiro graphs we produced at the beginning of the experiment which are photographed in figures 2 and 3. The “after exercise” spiro graph shows an increase in breathing rate as each of the waves represents one breath. There is also a vast difference in the gradient of each of the graphs which I have drawn diagonal straight lines across to clarify where I am referring to. The steeper gradient of the “after exercise” graph shows that more oxygen was absorbed by our test subject in the minute after exercise than the minute after resting. Finally on the “after exercise” graph the waves have a longer wavelength than the “at rest” graph. This means after one minute of exercise our test subject was taking in greater amounts of oxygen with each breath – so we can conclude from this that exertion on the body initiates more efficient aerobic breathing (or just more aerobic). We are limited to what conclusion we can derive from the last 2 results as the only thing we measured was breathing rate. All we can really conclude from these results is that exercise increases breathing rate; in order to provide our bodies with the extra oxygen needed to perform high energy processes.
Evaluation
There are a few things I would change if I were to repeat the experiment again. The first would be to use one method of data collection only; either the spirometer or counting manually – the spirometer being the preferable option, but only if it would work properly. This would ensure the results were reliable and accurate with respect to each other. Another would be to take the measurements consecutively as appose to letting the test subject rest between each interval of exercise – this would enable us to see the effect of exercise on respiration through various “stages” i.e. we could see more of the gradual affect over time. Using this method would be better because allowing our test subject to rest in between meant we were essentially repeatedly measuring the same thing.
The Lower Respiratory System
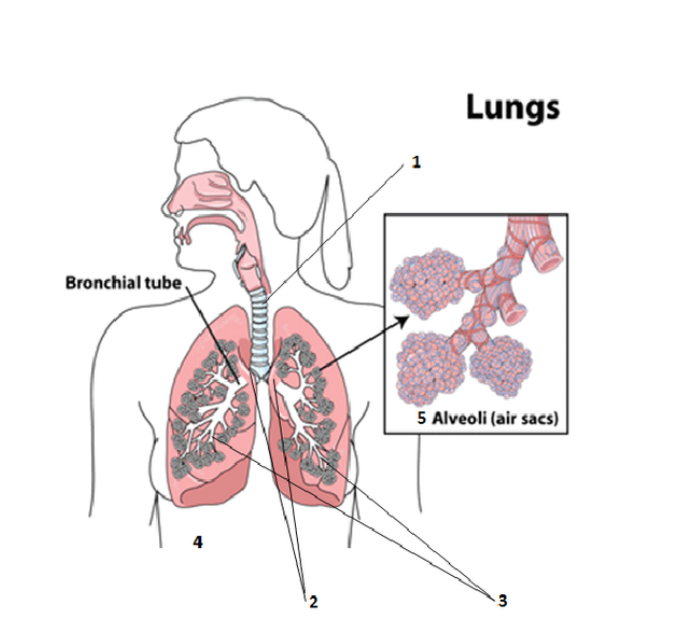
1.) Trachea
The trachea is made up of crescent shaped cartilage which is stacked like brick work right the way down so that it is constantly open and therefore able to fill with air on contact. The cells which line the trachea are ciliated stratified columnar epithelium; this allows it to stretch and extend a little with each breath taken – ensuring it doesn’t “snap”. The cilia and mucus produced by the goblet cells help to keep infection and other unwanted cellular invaders away from the lungs by catching or trapping dust, particles of food, bacteria etc. and forcing it back up the trachea and down the oesophagus to be digested. Its primary function, however, is to ensure there is always a clear airway for air to travel to and from the lungs, almost like an exchange surface.
2.) Bronchi
The trachea splits when it terminates and leads to two tubules to the left and right which are called bronchi (singularly bronchus). There are 3 “stages” to the bronchi as the tubes are made smaller and thinner and more suited to performing gaseous exchange. The primary bronchi are still made up of cartilage and the mucous membrane of the trachea extends to them as well. Further down, the primary bronchi noticeably changes structure again and the cartilage “rings” or crescents as I have named them become plates. This change is where the secondary bronchi begin. The secondary bronchi are thinner and smaller than the previous as they are closer to the lungs. There are 3 secondary bronchi in the right lung, but only 2 in the left. Finally in the last stage of the bronchi, the tertiary bronchi, cartilage is still present but there is a larger concentration of smooth muscle. The tertiary bronchi spread far around the lungs branching out in thin, gradually downsized airways. The bronchi help to moisten and heat up the air coming in before it reaches the alveoli.
3.) Bronchioles
At the end of the tertiary bronchi there are even tinier branches called bronchioles. The bronchioles are made up of smooth muscle tissue and contain no cartilage. Here the epithelium change structure and become simple columnar epithelial cells. The bronchioles subdivide like the bronchi, but into how many divisions is debatable, for the purpose of this assignment I will say two; terminal and respiratory. The group of bronchioles which are found closest to the alveoli can expand and contract to regulate airflow. They are called the respiratory bronchioles and they contain clara cells which secrete a protein called surfactant. Surfactant has many functions including lubricating the contact surfaces, detoxifying anything harmful in the lungs and maintaining airflow. In the respiratory bronchioles the ciliated stratified epithelium of the trachea has transformed into simple cuboidal as the surfaces prepare for gas exchange. The respiratory bronchioles sit between the terminal bronchioles and Alveolar ducts; it is their job to allow air and waste gas to cross between these surfaces through it semi permeable membrane.
4.) Diaphragm
The diaphragm is the organ in the respiratory system which keeps the chest and abdomen separate and is a thin sheet of skeletal muscle which presents in a dome shape. It flattens and expands in order to help “push” air in and out of the lungs.
5.) Alveoli:
The trachea is made up of crescent shaped cartilage which is stacked like brick work right the way down so that it is constantly open and therefore able to fill with air on contact. The cells which line the trachea are ciliated stratified columnar epithelium; this allows it to stretch and extend a little with each breath taken – ensuring it doesn’t “snap”. The cilia and mucus produced by the goblet cells help to keep infection and other unwanted cellular invaders away from the lungs by catching or trapping dust, particles of food, bacteria etc. and forcing it back up the trachea and down the oesophagus to be digested. Its primary function, however, is to ensure there is always a clear airway for air to travel to and from the lungs, almost like an exchange surface.
2.) Bronchi
The trachea splits when it terminates and leads to two tubules to the left and right which are called bronchi (singularly bronchus). There are 3 “stages” to the bronchi as the tubes are made smaller and thinner and more suited to performing gaseous exchange. The primary bronchi are still made up of cartilage and the mucous membrane of the trachea extends to them as well. Further down, the primary bronchi noticeably changes structure again and the cartilage “rings” or crescents as I have named them become plates. This change is where the secondary bronchi begin. The secondary bronchi are thinner and smaller than the previous as they are closer to the lungs. There are 3 secondary bronchi in the right lung, but only 2 in the left. Finally in the last stage of the bronchi, the tertiary bronchi, cartilage is still present but there is a larger concentration of smooth muscle. The tertiary bronchi spread far around the lungs branching out in thin, gradually downsized airways. The bronchi help to moisten and heat up the air coming in before it reaches the alveoli.
3.) Bronchioles
At the end of the tertiary bronchi there are even tinier branches called bronchioles. The bronchioles are made up of smooth muscle tissue and contain no cartilage. Here the epithelium change structure and become simple columnar epithelial cells. The bronchioles subdivide like the bronchi, but into how many divisions is debatable, for the purpose of this assignment I will say two; terminal and respiratory. The group of bronchioles which are found closest to the alveoli can expand and contract to regulate airflow. They are called the respiratory bronchioles and they contain clara cells which secrete a protein called surfactant. Surfactant has many functions including lubricating the contact surfaces, detoxifying anything harmful in the lungs and maintaining airflow. In the respiratory bronchioles the ciliated stratified epithelium of the trachea has transformed into simple cuboidal as the surfaces prepare for gas exchange. The respiratory bronchioles sit between the terminal bronchioles and Alveolar ducts; it is their job to allow air and waste gas to cross between these surfaces through it semi permeable membrane.
4.) Diaphragm
The diaphragm is the organ in the respiratory system which keeps the chest and abdomen separate and is a thin sheet of skeletal muscle which presents in a dome shape. It flattens and expands in order to help “push” air in and out of the lungs.
5.) Alveoli:
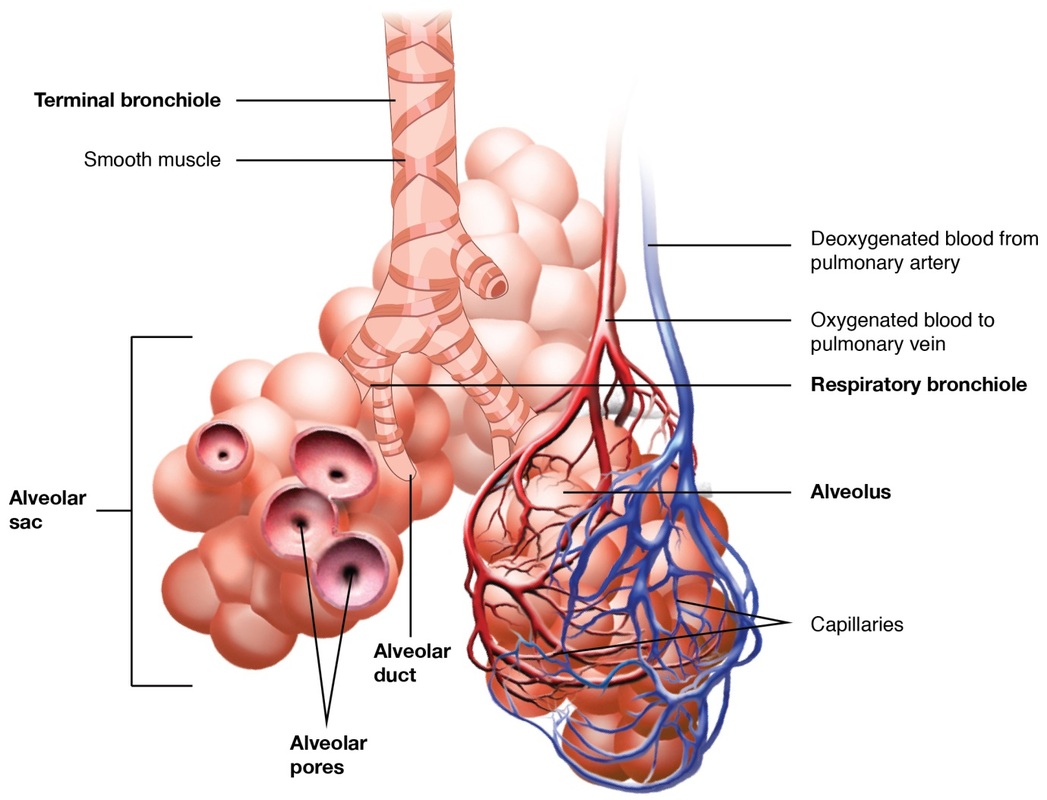
The alveoli of the lungs are designed perfectly for the purpose of gas exchange. One key design feature of the alveolus that enables such effective exchange of gases is its extremely thin, semi permeable membrane - a layer of one cell thick (simple) squamous epithelium gives the alveolus its structure. Simple squamous epithelium being only one cell thick means it has direct contact with both the lumen of the alveolus and the basement membrane. These epithelial cells, like the respiratory bronchioles, secrete a gelatinous substance called surfactant which helps stop the alveoli from collapsing by reducing surface tension and means less pressure is needed to inflate the lungs during inhalation. Surfactant is an extremely effective lubricant and stops friction occurring during respiratory processes which would be very painful. Its balloon or sphere type shape also gives the alveolus a really large surface area with minimal volume; this increased surface area ensures optimum levels of gases can diffuse between the alveolar membranes i.e. there is more space and therefore more opportunity for gas exchange. Each alveolar sac is encased in a network of blood vessels and capillaries which plays a vital role in sustaining oxygen supply in mammals. We need a constant supply of oxygen to stay alive so it is crucial that gases can diffuse into the blood stream from the lungs just short of instantaneously. Looking at the above diagram we can see these capillaries are linked to the pulmonary vein and artery which are coming from and going to the heart; thereby carrying nutrients to the body and from the body to the lungs. Between the alveoli and the surrounding blood capillaries there is a steep concentration gradient which helps speed up diffusion between the surfaces. Carbon dioxide molecules from the blood diffusing into the alveoli and oxygen molecules from the alveoli diffusing into the blood are each trying to reach an equilibrium between the surfaces which increases the rate at which they diffuse into their desired space. This gives an alternating effect where molecules are constantly trying to pass through the membrane to the other side which is very effective gas exchange.
